





If you're responsible for digital access, contact center performance, patient engagement, or clinical operations, the pressure is familiar. Calls spike early in the morning. Scheduling teams spend hours on tasks that should be automated. Patients expect answers after hours, but your staff can't scale around the clock. Clinicians want fewer clicks, not another disconnected tool.
That's why conversational AI has become more than a chatbot project. In healthcare, it's increasingly a way to reduce administrative friction, improve access, and support staff without adding another layer of operational complexity. The opportunity is real, but so is the failure mode. Many deployments look polished in a demo and break down once they hit live workflows, regulated data, and edge cases.
The organizations getting value from conversational AI for healthcare aren't starting with scripts and avatars. They're starting with system integration, governance, escalation design, and a clear operating model for where automation helps and where a human should take over.
Table of Contents
- Beyond the Buzzword Introduction to Healthcare AI
- What Is Conversational AI in a Healthcare Context
- Key Use Cases Across the Patient and Provider Journey
- Building a Secure and Integrated Technical Foundation
- Your Enterprise Implementation Roadmap and Governance
- Measuring Success and Avoiding Common Pitfalls
- The Future of Autonomous Healthcare Operations
Beyond the Buzzword Introduction to Healthcare AI
At 8:15 a.m., a patient messages about a referral, then asks whether a bill was processed, then mentions a prescription that still shows as pending. In many health systems, those requests split across the call center, the EHR, the billing platform, and the pharmacy workflow. Staff spend time chasing context across disconnected tools. Patients experience delay, repetition, and dropped handoffs.
That is the operating problem conversational AI needs to solve in healthcare.
The strategic value is not a nicer chat interface. It is the ability to reduce avoidable labor, shorten response times, and keep routine service work from overwhelming teams that are already stretched. Industry coverage from McKinsey on generative AI in healthcare reflects why executive interest keeps rising. The opportunity is tied to administrative complexity, documentation burden, and patient access friction, not novelty.
For enterprise buyers, the central question is narrower and harder. Can the system connect to source systems, apply policy controls, support audit requirements, and improve a workflow that matters to operations or margin?
That standard rules out a lot of weak projects.
The strongest early wins usually come from high-volume service workflows with clear boundaries. Appointment management, patient intake questions, benefits checks, status updates, refill routing, and internal staff support all fit that pattern. Cleffex on virtual patient care points to the same broad shift toward digital patient interaction, but the enterprise lesson is more specific. Value comes from fitting AI into the operating model, not from adding a bot to the website.
I have seen healthcare organizations get stuck when they start with the model demo instead of the workflow. A polished assistant can still fail in production if it cannot read the right data, trigger the next action, or escalate safely to a human. In regulated environments, those gaps become governance issues quickly.
So the conversation has to move beyond feature lists. The implementation case for conversational AI in healthcare rests on three pillars: deep integration with systems of record, governance that is active in day-to-day operations, and a roadmap tied to measurable ROI. Without those pieces, adoption stays shallow and risk rises faster than value.
What Is Conversational AI in a Healthcare Context
In healthcare, conversational AI isn't just a nicer chat window. It's a system that can understand intent, manage dialogue, retrieve the right information, trigger actions in connected systems, and hand off to staff when confidence or policy requires it.
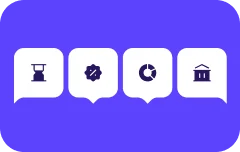
Older healthcare bots were usually rule trees with narrow decision paths. They worked for a short list of scripted FAQs, then failed the moment a patient phrased something differently or asked a follow-up question. Modern systems are closer to an orchestration layer. They combine natural language understanding, workflow logic, enterprise integration, and increasingly, grounded generation.
From scripted bot to operational assistant
A useful analogy is this. A legacy chatbot is like a keypad menu with better wording. Modern conversational AI is closer to a service coordinator that can listen, check systems, guide a user, and complete the next step.
That distinction matters in healthcare because conversations rarely stay static. A patient starts by asking about a bill, then mentions a missed appointment, then asks whether a refill request went through. A clinician asks for a note summary, then wants a medication list, then needs the next action documented in the right workflow. A healthcare-grade assistant needs context, not just canned answers.
Among healthcare payers and providers actively using AI, conversational AI is the leading workload at 54%, and chatbots and agents are among the top GenAI use cases at 53%, according to Master of Code's healthcare AI statistics roundup. That's a strong sign that conversational systems are already central to real healthcare AI programs, not side experiments.
Patient-facing and staff-facing use both matter
The market often talks about patient chatbots because they're visible. But the bigger enterprise story includes both patient experience and employee experience.
On the patient side, conversational AI helps with always-on support, intake, reminders, navigation, and access. On the staff side, it supports repetitive administrative work, information retrieval, workflow guidance, and documentation-adjacent tasks. When teams evaluate the category narrowly, they often miss the compound value that comes from supporting both fronts at once.
For a useful overview of how virtual assistants fit into care delivery workflows, Cleffex on virtual patient care is a practical companion read.
A healthcare chatbot becomes strategically important when it stops being a digital front door and starts acting as an intelligent workflow layer across patient and staff interactions.
The practical takeaway is simple. Conversational AI for healthcare should be defined by what it can do inside your operating environment, not by whether it can hold a smooth conversation.
Key Use Cases Across the Patient and Provider Journey
At 7:10 a.m., a patient tries to reschedule a follow-up after a medication change. At 7:12, a nurse wants the latest discharge instruction. At 7:15, the call center is already stacking hold times. These are not separate problems. They are one operational chain, and conversational AI adds value only when it helps that chain move faster with fewer handoffs and fewer errors.
That is the right lens for use cases. Start with the work that must get done across the patient and provider journey, then identify where a conversational interface can remove queue time, reduce manual effort, or improve consistency. Enterprise teams get the strongest returns when they map use cases to existing workflows, owners, systems, and controls instead of buying around a feature list.
Non-clinical workflows usually deliver the first wins
Most health systems should begin with administrative journeys. The risk is lower, the volume is high, and the ROI is easier to measure in containment rates, reduced call burden, faster access, and fewer abandoned tasks.
| Category | Primary Goal | Example Use Cases | Key Value Driver |
|---|---|---|---|
| Non-clinical | Improve access and reduce administrative load | Appointment scheduling, rescheduling, insurance verification, FAQs, reminders, portal support, billing inquiry routing | Faster service, lower call burden, fewer manual touches |
| Clinical | Support care delivery and workflow coordination | Medication reminders, symptom intake support, EHR information retrieval, note support, follow-up guidance | Better continuity, stronger workflow support, more timely intervention |
In these non-clinical flows, completion matters more than conversation quality. The assistant should confirm identity, capture intent, apply scheduling and routing rules, and finish the task. If it creates extra turns, sends users into a portal dead end, or fails to transfer context to staff, it adds cost instead of removing it.
Common high-value examples include:
- Scheduling and rescheduling: Verify provider, specialty, location, visit type, and slot rules before presenting options.
- Insurance and administrative checks: Guide patients through pre-visit requirements without forcing them across separate channels.
- Reminder and follow-up flows: Confirm attendance, collect simple updates, and send exceptions to the right team.
- Patient FAQ support: Answer repeat operational questions using governed content that has an owner and a review cycle.
For a broader view of common deployment patterns, this overview of healthcare chatbot use cases is a useful reference.
Clinical support creates value, but scope has to be tighter
Clinical workflows can produce significant gains, but they require narrower use-case design, stronger review processes, and clearer escalation rules. In practice, the safest deployments focus on bounded tasks that support care teams rather than replace clinical judgment.
The patterns that usually hold up in production are straightforward:
- Medication and care-plan support: Reminders, adherence check-ins, and structured follow-up questions tied to approved protocols.
- Care navigation: Step-by-step guidance after discharge, before procedures, or during chronic care programs when content is reviewed and current.
- Internal clinical workflow support: Fast retrieval of approved patient or policy information for staff inside controlled environments.
- Documentation support: Speech-to-text and summarization workflows that save clinician time before final review. Teams assessing this area should also look at how speech recognition healthcare fits into documentation operations.
A practical benchmark is simple. If the assistant can complete the task with approved content, known data inputs, and a clear escalation path, it is a strong candidate. If the use case depends on open-ended medical advice, uncertain context, or invisible business rules, the design usually breaks under real-world demand.
Clinical use cases also fail for governance reasons. Teams launch symptom support without defining when to route to a nurse line. They add note summarization without clarifying reviewer responsibility. They expose EHR lookups without enough role-based access control. The technology is rarely the only issue. Operating discipline is what separates a useful clinical assistant from a risky one.
The best healthcare assistants have a defined role, bounded authority, and a reliable handoff path.
The strategic point is broader than chatbot functionality. Across the patient and provider journey, conversational AI works best as an operational service layer that completes tasks, routes exceptions, and supports staff inside established workflows. That is how organizations move from isolated pilots to measurable enterprise value.
Building a Secure and Integrated Technical Foundation
Most healthcare AI problems that look like model problems are architecture problems. The assistant sounds capable in a sandbox, but it can't see the right data, can't trigger the right action, can't verify identity reliably, or can't operate within compliance controls. That's why the technical foundation matters more than the demo.
Architecture decides whether the bot is useful
The core requirement is tight integration with systems of record. Master of Code's discussion of conversational AI in healthcare architecture makes this point clearly: effective conversational AI in healthcare requires tight integration with core systems like EHRs and patient portals. That's what turns a simple chatbot into an operational tool that can provide context-aware, personalized actions based on live enterprise data.
In practice, that means the assistant should be able to do things such as:
- Read current context: Upcoming appointments, medication lists, care pathway status, and approved content.
- Trigger workflow actions: Schedule, route, notify, document, or escalate without forcing a user into another channel.
- Ground responses in trusted data: Use retrieval patterns so the model responds from the current enterprise context rather than generic memory.
- Support channel continuity: A patient shouldn't have to repeat the same issue across web chat, voice, SMS, or portal interactions.
RAG becomes useful, but only when the retrieval layer is well-governed. Grounding a response in stale, duplicated, or poorly permissioned data doesn't improve safety. It just makes the wrong answer sound more authoritative.
Speech also matters. Many healthcare interactions are faster by voice than by form. For teams evaluating how voice capture supports clinical and administrative workflows, speech recognition healthcare offers a practical view of where voice technology fits.
Security and operational control are product requirements
Healthcare buyers sometimes treat compliance as a procurement checkbox. That's a mistake. Security, auditability, access control, and data handling policies shape what you can safely automate.
The minimum bar should include clear controls around identity, role-based access, logging, protected data handling, model behavior policies, and integration governance. Operationally, you also need testing environments, release discipline, fallback paths, and escalation controls. A bot that can answer elegantly but can't be audited isn't enterprise-ready.
For platform evaluation, it helps to benchmark capabilities against an enterprise-grade security model for conversational AI. The right standard isn't aesthetic polish. It's whether the platform can operate safely inside regulated workflows over time.
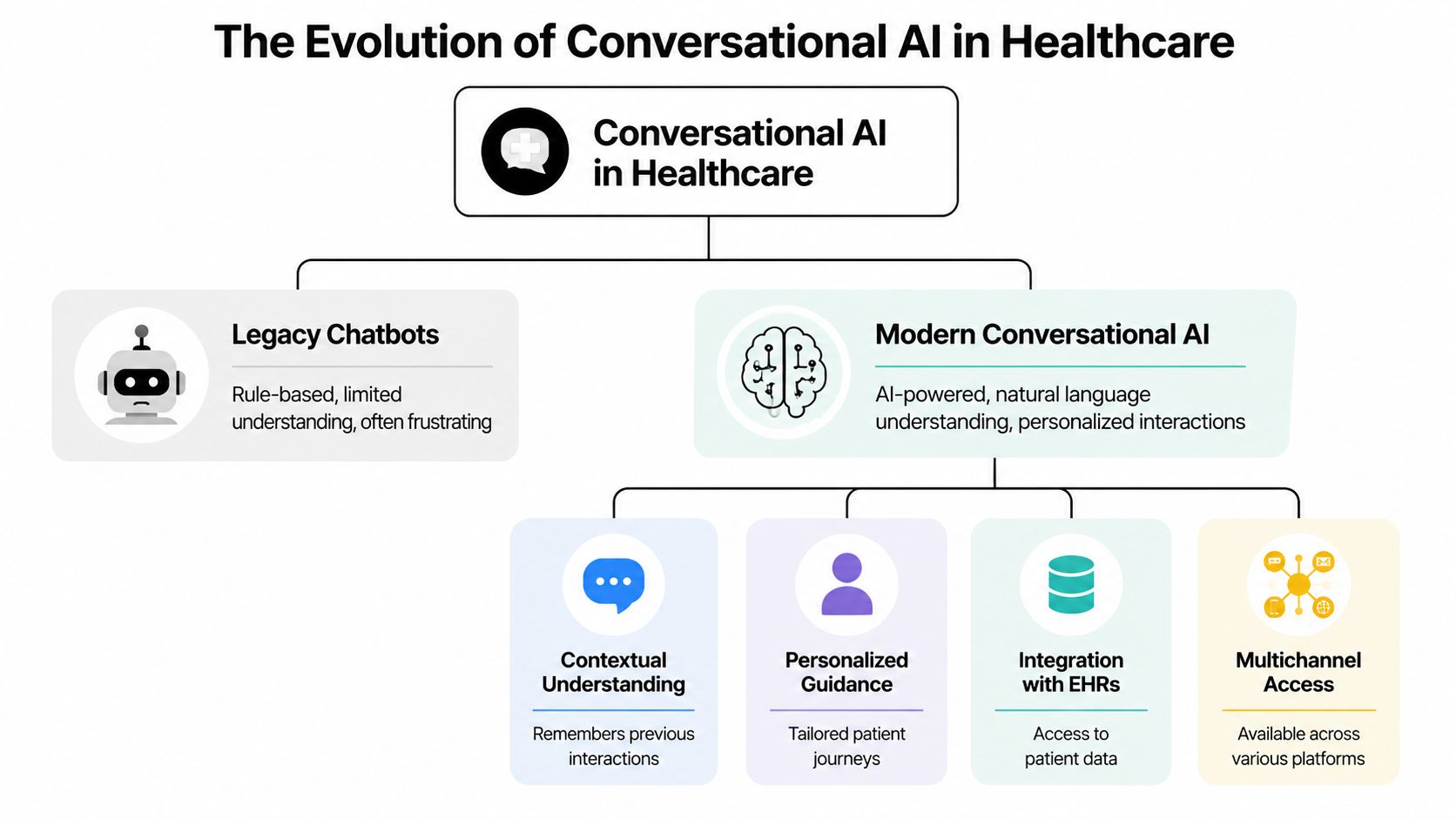
One practical pattern is to separate the layers:
- Conversation layer: Handles intent, dialogue, channel behavior, and response composition.
- Retrieval and orchestration layer: Fetches approved knowledge, enforces rules, and coordinates actions.
- System integration layer: Connects to EHR, CRM, scheduling, billing, and identity services.
- Governance layer: Controls prompts, permissions, auditing, testing, and exception handling.
Yellow.ai is one example of a platform in this category. It supports agentic AI workflows, multi-LLM orchestration, omnichannel deployment, and enterprise compliance controls relevant to healthcare environments. The larger point, though, is platform fit. Choose the system that aligns with your integration depth, governance needs, and operating model.
Your Enterprise Implementation Roadmap and Governance
Healthcare organizations usually get into trouble when they treat conversational AI as a channel project. It isn't. It's an operating model change that touches service design, compliance, clinical safety, data architecture, and workforce workflows.
Start with business pain not model capability
The most reliable rollout sequence starts with a narrow, high-friction workflow that already has clear owners and measurable pain. Appointment access, patient communication triage, internal service desk support, and reminder workflows are common starting points because they're operationally meaningful and easier to govern.
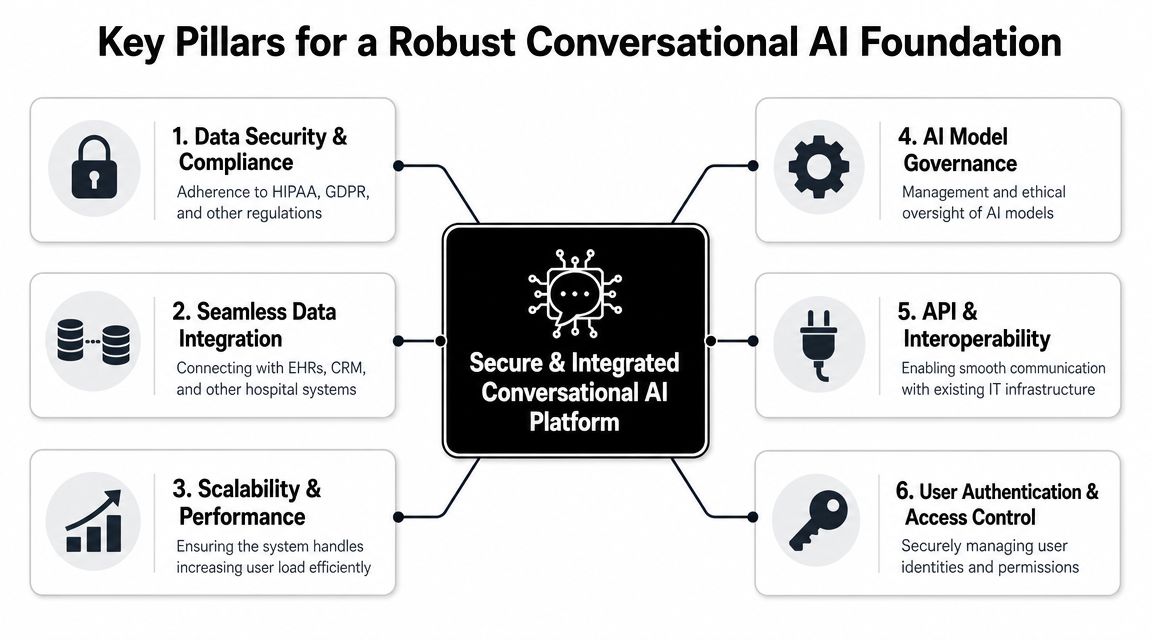
A practical roadmap usually looks like this:
Discovery and prioritization
Map where demand is high, manual effort is repetitive, and workflow rules are clear. Separate low-risk service automation from higher-risk clinical support early.Workflow and policy design
Define what the assistant may do, what data it can access, what it must never do, and when it must hand off to a human.Pilot with constrained scope
Launch with a specific department, patient group, or use case. Limit channels and integrations at first if that improves control.Expand only after review
Scale after teams validate quality, operational fit, escalation behavior, and governance performance in production.
This video gives a useful visual frame for how teams think about phased healthcare AI deployment:
A peer-reviewed roadmap summarized in this PubMed Central article on equitable conversational AI implementation outlines a 10-stage process that includes co-production, explicit safety measures, testing, healthcare integration, auditing, maintenance, and termination. That's the right level of seriousness for healthcare. You aren't deploying a script. You're introducing an actor into a live service environment.
Governance has to be active not symbolic
Most enterprises already have governance committees. That doesn't mean they have effective AI governance. In practice, a healthcare conversational AI program needs a cross-functional operating group that can make real decisions quickly.
That group should include leaders from:
- Clinical operations: To define acceptable workflow roles and escalation boundaries.
- IT and architecture: To approve integration patterns, identity controls, and data flow design.
- Compliance and privacy: To review data handling, consent implications, and audit needs.
- Contact center or patient access teams: To shape real-world service logic and handoff paths.
- Product or digital leaders: To maintain roadmap discipline and adoption accountability.
Don't ask governance teams to review a finished bot. Ask them to help define the operating rules before build starts.
Good governance also means lifecycle management. You need regular review of intent coverage, failed interactions, escalation rates, knowledge freshness, and policy exceptions. Healthcare workflows change. If the assistant doesn't change with them, it degrades unnoticed until staff stop trusting it.
Measuring Success and Avoiding Common Pitfalls
If your scorecard only tracks containment, you'll misread the program. A healthcare assistant can deflect conversations and still create more downstream work, more patient confusion, or more risk. The point is not to keep humans out of the loop at all costs. The point is to complete the right work safely and efficiently.
Measure workflow outcomes not just bot activity
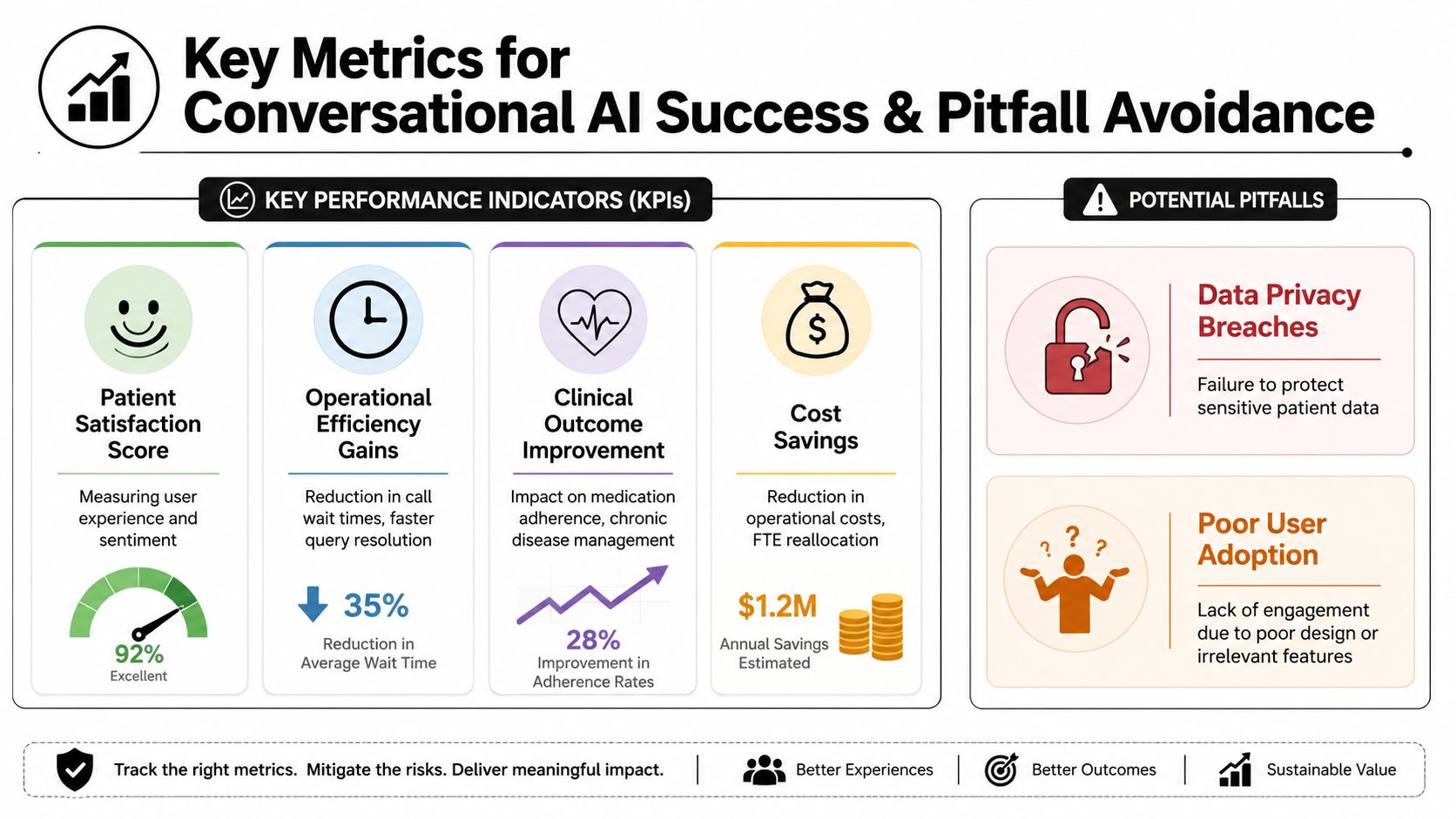
The best KPI set blends operational, experience, and risk indicators.
Track measures such as:
- Operational completion: Did the system finish the appointment, verification, routing, or reminder task?
- Escalation quality: When the bot handed off, did the human receive context or start from zero?
- Patient experience: Did users get a clear answer and next step without channel switching?
- Staff impact: Did front-desk, contact center, or care teams save meaningful time on repetitive work?
- Governance health: Were responses grounded, auditable, and aligned to approved workflow boundaries?
For clinical-adjacent use cases, add outcome-oriented review. Don't just ask whether the system answered. Ask whether it supported the intended care process without introducing ambiguity or delay.
Common failure patterns in healthcare deployments
Many teams know the obvious risks, such as privacy and hallucinations. The subtler failures are usually strategic.
One major one is equity. This PLOS Digital Health paper on equitable conversational AI argues that equitable design should begin with a needs assessment that identifies specific disparities, includes co-design with underrepresented communities, and defines target health outcomes upfront. That matters because a bot that works for digitally fluent, English-dominant users may underperform for the very populations that face the biggest access barriers.
Other common pitfalls include:
- Weak source data: If scheduling logic, FAQs, or pathway content are inconsistent, the assistant will expose the inconsistency faster.
- No clear role boundary: Users assume the bot can do more than it should, especially in symptom or care-navigation contexts.
- Poor handoff design: Staff receive an escalated conversation with missing context, then trust drops on both sides.
- Fragmented ownership: Digital owns the interface, IT owns integrations, operations owns outcomes, and no one owns the full journey.
- Static launch mindset: Teams deploy once, then underinvest in tuning, testing, and governance review.
Useful ROI in healthcare includes fewer manual touches, lower service friction, better consistency, and reduced operational risk. Cost reduction is only part of the picture.
The strongest programs treat measurement as a control system. They use KPIs to catch drift, not just to justify the project after launch.
The Future of Autonomous Healthcare Operations
The long-term shift isn't toward more bots. It's toward more autonomous operations, where conversational interfaces become the front end to coordinated enterprise action.
That doesn't mean removing humans from healthcare. It means removing humans from repetitive administrative work that doesn't require empathy, judgment, or clinical nuance. Staff should spend less time on routing, chasing status, re-entering information, and repeating standard instructions. They should spend more time on exception handling, relationship-driven support, and care decisions.
The healthcare organizations that get there won't do it by buying a chatbot and hoping adoption follows. They'll build conversational AI for healthcare as infrastructure. That means system integration, policy-driven orchestration, governed knowledge, and a service model that defines when automation acts and when people step in.
If you're also evaluating how generative capabilities fit into that roadmap, this guide to generative AI in healthcare is a useful next read.
The next generation of healthcare operations will feel less like a queue and more like coordinated flow. Patients will ask, confirm, reschedule, check, and follow up through natural conversation. Staff will work with systems that surface the right context and complete the next action. The organizations that design for that future now will move faster, serve more reliably, and create a better experience for both patients and teams.
Yellow.ai provides an enterprise agentic AI platform that healthcare organizations can evaluate for patient support, scheduling, workflow automation, and secure omnichannel deployment. If you're building a roadmap for conversational AI in a regulated environment, it's worth assessing platforms based on integration depth, governance controls, compliance posture, and how quickly they can move from pilot to operational scale.



